Volume 9, Issue 4 (Winter 2024)
JMIS 2024, 9(4): 382-399 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Dorrani M, Zangoui S, Alborzi R. Comparison of the Actual Cost of Global Surgeries in the Hospitals Affiliated to Birjand University of Medical Sciences With the Government-approved Tariffs in 2021. JMIS 2024; 9 (4) :382-399
URL: http://jmis.hums.ac.ir/article-1-460-en.html
URL: http://jmis.hums.ac.ir/article-1-460-en.html



Management of Organization Development and Administrative Transformation, Vice President of Management and Resources Development, Birjand University of Medical Sciences, Birjand, Iran.
Full-Text [PDF 5400 kb]
(1999 Downloads)
| Abstract (HTML) (3201 Views)
Full-Text: (7109 Views)
Introduction
Reimbursement methods in the health system are one of the influencing factors in the behavior of service providers and the quality of services. Different countries use different reimbursement methods in their health system. One of the conventional methods for reimbursing hospital services is the diagnosis-related group (DRG)-based reimbursement system. The common payment system in Iranian hospitals is the retrospective reimbursement system, and the prospective reimbursement system is used only for a limited number of medical procedures. This reimbursement system has been adapted from the DRG-based system, which has been adjusted and notified to all hospitals since 1998 under the title of “global tariffs for common surgical procedures”, separated based on the evaluation grades of hospitals. Currently, this system is used for reimbursement in the second and third levels of service provision in Iran, which has differences with the DRG-based system. The primary and secondary diagnoses that have comprehensively been mentioned in the DRG-based system, do not exist in the global tariffs system. The variables of age, sex, and many factors affecting diseases have not been considered in the global tariffs system, which can be the disadvantage of this system compared to the DRG-based system. This study aims to compare the actual global surgery costs in the hospitals affiliated to Birjand University of Medical Sciences (BUMS) with government-approved tariffs.
Methods
This is a retrospective study that was conducted in 2021 in 11 teaching hospitals affiliated to BUMS. The study population included all the global surgery bills available in the information systems of hospitals. The criterion for entering the study was the presence of sufficient samples (at least 10 bills) from each of the performed global surgeries. The sampling was done using a non-probability method. Out of 91 surgical procedures, 57 most frequent surgical procedures were included (equivalent to 63% of all global surgical procedures). The extracted data were compared with the government-approved tariffs. Mean and percentage were used to describe data, and Excel software version 2016 was used for data analysis.
Results
Out of 15,616 examined cases, 65% were in the gynecology and obstetrics group, 19% in the general surgery group, and 16% in the ENT and eye surgery group. Based on the findings, in 52% of the global surgeries, the global income was lower than the average actual cost, while in 48% of the cases, the hospitals benefited from the costs of surgery. The average actual costs for surgeries and their difference with the global tariffs are presented in Table 1.
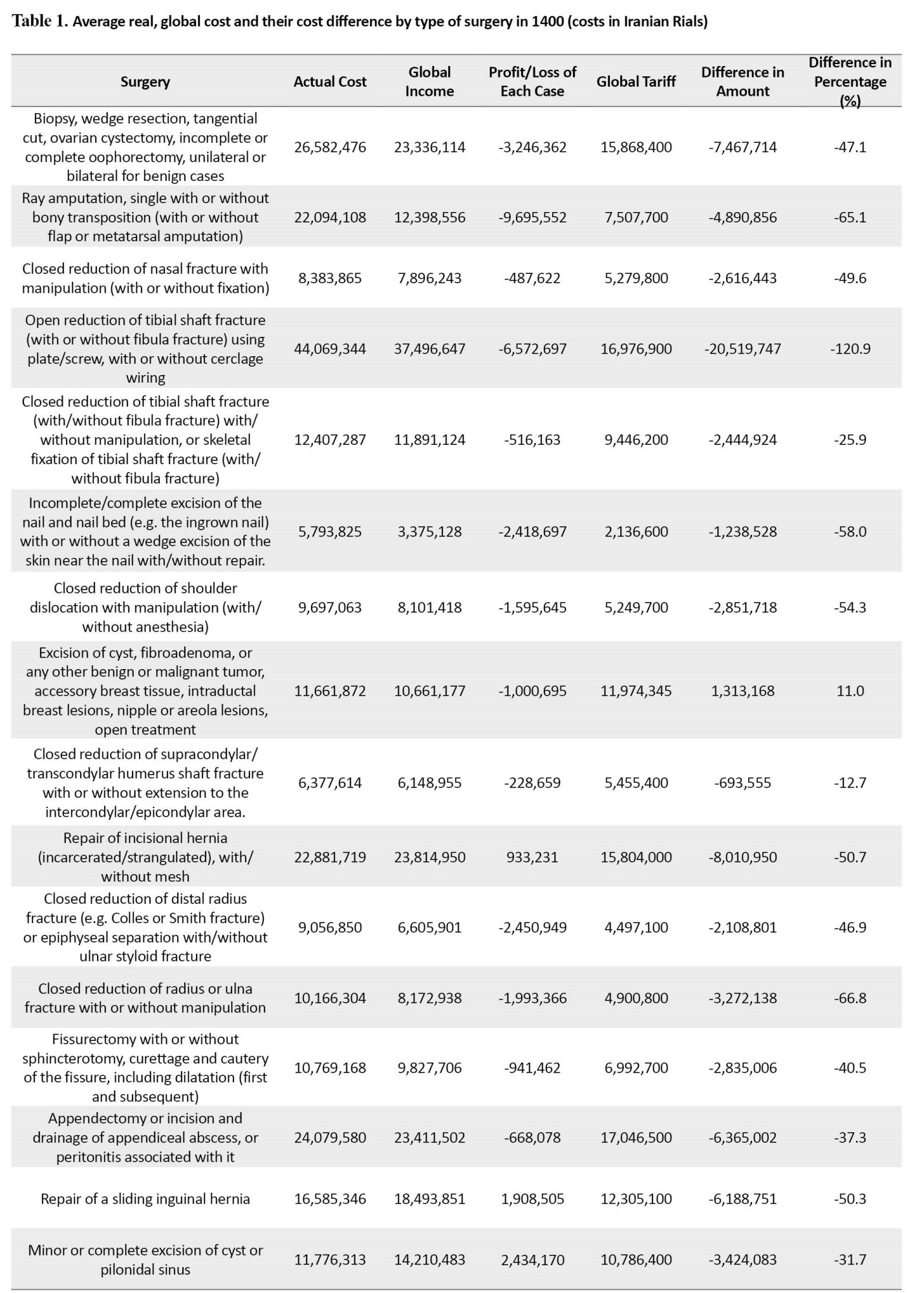

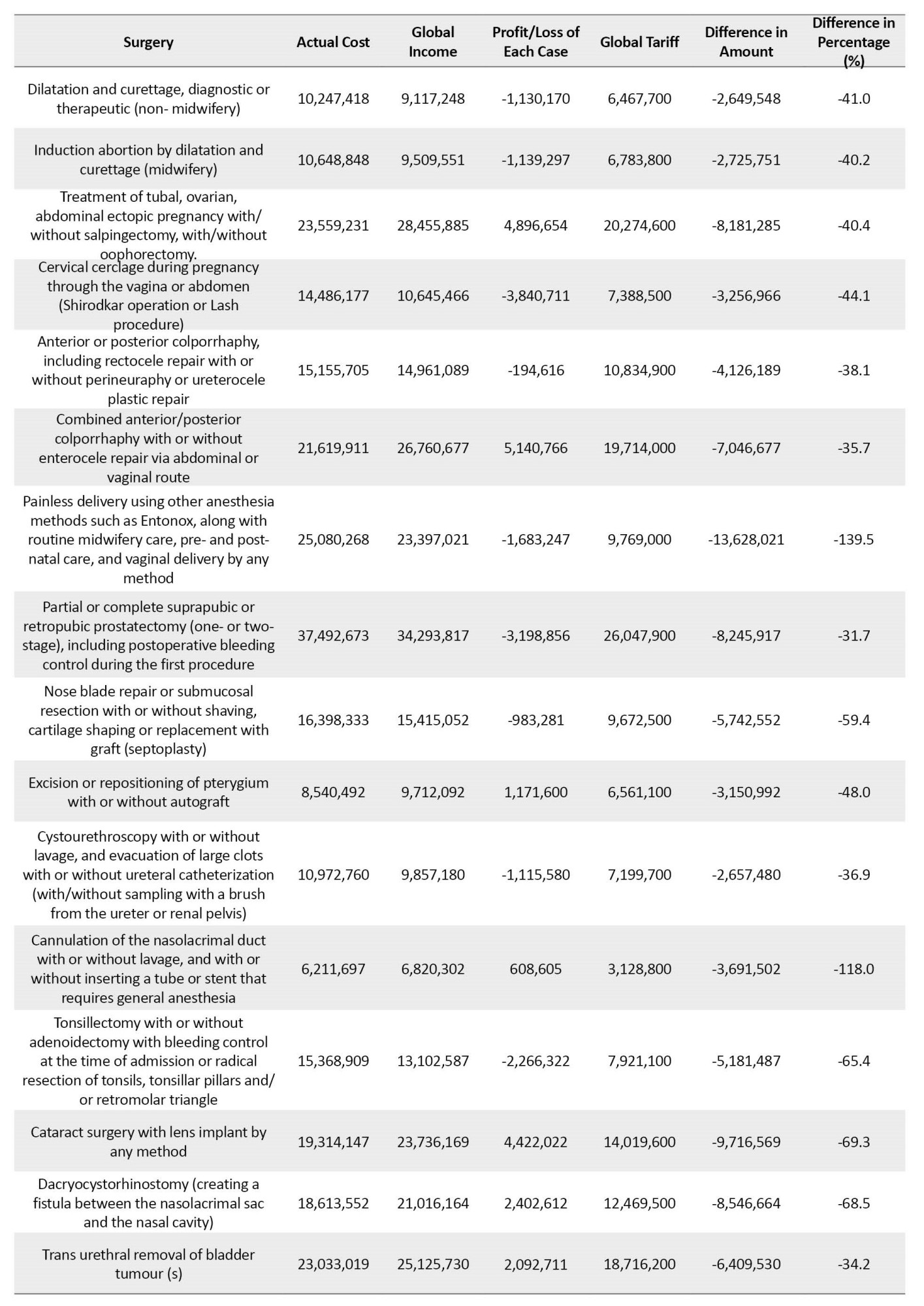

In 56 cases of global surgery, the fee was 12-139% higher than the approved global tariff. In 23 surgeries, the difference was more than 50%. The highest percentage of loss was related to the “painless delivery using other anesthesia methods such as Entonox, along with routine midwifery care, pre- and post-delivery care, and vaginal delivery by any method.” (139%). The highest amount of loss was related to “bone fixation for proximal femoral fractures in the neck, through the skin or open surgery” (281,108,44 Iranian Rials per surgery).
Conclusion
The results of this study showed that the costs of global surgical services in the hospitals affiliated to the BUMS are higher than their approved global tariffs. Therefore, the hospitals do not achieve profit margin. Therefore, to overcome the loss-making situation and justify the costs of global inpatient services in these hospitals, the officials should pay more attention to the cost management of inpatient services every year while paying attention to the amount of the approved tariffs for global services, and try to reduce their costs as much as possible and as long as the quality of the hospital services is not harmed, by using standard methods such as rational prescription of drugs and equipment and commitment to guidelines. On the other hand, due to the disproportion between the approved tariffs and the costs of global services in hospitals, the Ministry of Health and Medical Education and other relevant trustees should review the global tariffs in a timely manner and in accordance with the changes and growth of inflation.
Ethical Considerations
Compliance with ethical guidelines
This article is taken from the research plan approved by the Vice-Chancellor. Research and technology of Birjand University of Medical Sciences (No.: 5806, Ethics Code IR.BUMS.REC.1401.148) and with the cooperation of the officials of the revenue unit of 11 hospitals. The province is done.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design: Somia Zengoui; Data Collection and data analysis: Somia Zengoui and Maryam Durrani; Preparation of report research: Maryam Durrani; Coordination for obtaining reports and data from hospitals: Ruhollah al-Barzi.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors appreciate the support of Vice president of research and technology of the Birjand University of Medical Sciences.
Reimbursement methods in the health system are one of the influencing factors in the behavior of service providers and the quality of services. Different countries use different reimbursement methods in their health system. One of the conventional methods for reimbursing hospital services is the diagnosis-related group (DRG)-based reimbursement system. The common payment system in Iranian hospitals is the retrospective reimbursement system, and the prospective reimbursement system is used only for a limited number of medical procedures. This reimbursement system has been adapted from the DRG-based system, which has been adjusted and notified to all hospitals since 1998 under the title of “global tariffs for common surgical procedures”, separated based on the evaluation grades of hospitals. Currently, this system is used for reimbursement in the second and third levels of service provision in Iran, which has differences with the DRG-based system. The primary and secondary diagnoses that have comprehensively been mentioned in the DRG-based system, do not exist in the global tariffs system. The variables of age, sex, and many factors affecting diseases have not been considered in the global tariffs system, which can be the disadvantage of this system compared to the DRG-based system. This study aims to compare the actual global surgery costs in the hospitals affiliated to Birjand University of Medical Sciences (BUMS) with government-approved tariffs.
Methods
This is a retrospective study that was conducted in 2021 in 11 teaching hospitals affiliated to BUMS. The study population included all the global surgery bills available in the information systems of hospitals. The criterion for entering the study was the presence of sufficient samples (at least 10 bills) from each of the performed global surgeries. The sampling was done using a non-probability method. Out of 91 surgical procedures, 57 most frequent surgical procedures were included (equivalent to 63% of all global surgical procedures). The extracted data were compared with the government-approved tariffs. Mean and percentage were used to describe data, and Excel software version 2016 was used for data analysis.
Results
Out of 15,616 examined cases, 65% were in the gynecology and obstetrics group, 19% in the general surgery group, and 16% in the ENT and eye surgery group. Based on the findings, in 52% of the global surgeries, the global income was lower than the average actual cost, while in 48% of the cases, the hospitals benefited from the costs of surgery. The average actual costs for surgeries and their difference with the global tariffs are presented in Table 1.
In 56 cases of global surgery, the fee was 12-139% higher than the approved global tariff. In 23 surgeries, the difference was more than 50%. The highest percentage of loss was related to the “painless delivery using other anesthesia methods such as Entonox, along with routine midwifery care, pre- and post-delivery care, and vaginal delivery by any method.” (139%). The highest amount of loss was related to “bone fixation for proximal femoral fractures in the neck, through the skin or open surgery” (281,108,44 Iranian Rials per surgery).
Conclusion
The results of this study showed that the costs of global surgical services in the hospitals affiliated to the BUMS are higher than their approved global tariffs. Therefore, the hospitals do not achieve profit margin. Therefore, to overcome the loss-making situation and justify the costs of global inpatient services in these hospitals, the officials should pay more attention to the cost management of inpatient services every year while paying attention to the amount of the approved tariffs for global services, and try to reduce their costs as much as possible and as long as the quality of the hospital services is not harmed, by using standard methods such as rational prescription of drugs and equipment and commitment to guidelines. On the other hand, due to the disproportion between the approved tariffs and the costs of global services in hospitals, the Ministry of Health and Medical Education and other relevant trustees should review the global tariffs in a timely manner and in accordance with the changes and growth of inflation.
Ethical Considerations
Compliance with ethical guidelines
This article is taken from the research plan approved by the Vice-Chancellor. Research and technology of Birjand University of Medical Sciences (No.: 5806, Ethics Code IR.BUMS.REC.1401.148) and with the cooperation of the officials of the revenue unit of 11 hospitals. The province is done.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Study design: Somia Zengoui; Data Collection and data analysis: Somia Zengoui and Maryam Durrani; Preparation of report research: Maryam Durrani; Coordination for obtaining reports and data from hospitals: Ruhollah al-Barzi.
Conflicts of interest
The authors declared no conflict of interest.
Acknowledgements
The authors appreciate the support of Vice president of research and technology of the Birjand University of Medical Sciences.
References
- Kavosi Z, Jafari A, Keshtkaran V, Pourahmadi E. Estimating willingness to pay for an improved service delivery to patients referring Namazi Hospital Chemical Therapy Ward in Iran using contingent valuation. Asian Pac J Cancer Prev. 2018; 19(7):1817-23. [DOI:10.22034/APJCP.2018.19.7.1817] [PMID] [PMCID]
- Zare Askari A, Mir Mohammadkhani M, Shahab MR, Ebrahimian AA. [Comparison of global inpatient services costs with approved tariffs in niknafs obstetrics and gynecology hospital in Rafsanjan in 2019: A descriptive study (Persian)]. J Rafsanjan Univ Med Sci. 2022; 20(10):1117-28. [DOI:10.52547/jrums.20.10.1117]
- Jacobs P, Rapoport J. The economics of health and medical care. Sudbury: Jones and Bartlett Publishers; 2004. [Link]
- Janati A, Farough Khosravi M, Imani A, Javadzadeh A, Mazhar Gharamaleki M, Khosravi M, et al. Cost analysis of eye surgeries and comparison with approved governmental tariffs. Health Scope. 2017. 6(2):e39948. [DOI:10.5812/jhealthscope.39948]
- Kalhor R, Amini S, Emami M, Kakasoltani K, Rhamani N, Kalhor L. Comparison of the ministry of health's tariffs with the cost of radiology services using the activity-based costing method. Electron Physician. 2016; 8(2):2018-24. [DOI:10.19082/2018] [PMID] [PMCID]
- Zarei E. Hashemi M. Daneshkohan A. Kakemam E. Does the approved tariff cover the actual cost of global surgical procedures? Cost Effectiveness and Resource Allocation. 2020; [Unpublished]. [DOI:10.21203/rs.2.24251/v1]
- Karamouz M, Zahraie B, Kerachian R, Jaafarzadeh N, Mahjouri N. Developing a master plan for hospital solid waste management: A case study. Waste Manag. 2007; 27(5):626-38. [DOI:10.1016/j.wasman.2006.03.018] [PMID]
- Ebrahimipour H, Pourahmadi E, Badiee Aval S, Rezazadeh A. Comparison of the charges of 10 selected surgeries in Imam Reza Hospital with their official global prices. J Research Health. 2020; 10(5):319-28. [DOI:10.32598/JRH.10.5.1712.1]
- Kermani B, Gharsi M, Ghanbari B, Sarabi Asiabar A, Atefi Manesh P, Baniasadi A, et al. [The relationship between the levels of patient care and length of stay in hospital. (Persian)]. Shefaye Khatam. 2015. 3(S1):32-40. [DOI:10.18869/acadpub]
- Ergün FA, Ağirbaş I, Kuzu I. Activity-based costing for pathology examinations and comparison with the current pricing system in Turkey. Turk Patoloji Derg. 2013; 29(1):1-14. [DOI:10.5146/tjpath.2013.01141] [PMID]
- Lotter O, Amr A, Chiarello P, Bihler M, Schaller HE, Stahl S. Diagnosis -related groups in hand surgery -a comparison of six european countries. GMS Ger Med Sci. 2012. 10(8):1-10. [DOI:10.3205/000159]
- Aboutorabi A, Radinmanesh M, Rezapour A, Afshari M, Taheri G. A comparison of global surgery tariffs and the actual cost of bills at Hazrate Rasoole Akram educational and medical center. Cost Eff Resour Alloc. 2020; 18:38. [DOI:10.1186/s12962-020-00232-w] [PMID] [PMCID]
- Negrini D, Kettle A, Sheppard L, Mills GH, Edbrooke DL. The cost of a hospital ward in Europe: Is there a methodology available to accurately measure the costs? J Health Organ Manag. 2004; 18(2-3):195-206.[DOI:10.1108/14777260410548437] [PMID]
- Rashidian A, Radinmanesh M, Afshari M, Arab M, Shahinfar Z. The comparison of the global surgery fees and the actual cost in two educational hospitals affiliated to Tehran University of Medical Sciences. Evid Based Health Policy Manag Econ. 2018; 2(4):239-48. [DOI:10.18502/jebhpme.v2i4.275]
Type of Study: Research |
Subject:
Special
Received: 2023/05/17 | Accepted: 2023/11/13 | Published: 2024/01/1
Received: 2023/05/17 | Accepted: 2023/11/13 | Published: 2024/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Us
Post Address: Bandar Abbas, Imam Hossein Boulevard, campus of University of Medical Sciences, School of Nursing and Midwifery.
Tel: +(98) 763 331 7723
Cell Phone: +(98) 939 654 9816
jmis hums.ac.ir
hums.ac.ir